

STORY AT-A-GLANCE
- Scientists warn repeated COVID boosters may result in lowered immunity through a process known as “original antigenic sin” or “immune imprinting”
- Original antigenic sin describes how your first exposure to a virus shapes the outcome of subsequent exposures to antigenically related strains. The end result is that you become increasingly prone to symptomatic infections
- Data from the U.S. Centers for Disease Control and Prevention confirm that people who got two or three COVID jabs are MORE likely to get ill with COVID six to eight months after the last dose than had they gotten none
- Health authorities are potentially worsening matters further by pushing people to simultaneously get the updated bivalent COVID booster and a quadrivalent flu vaccine this fall
- The COVID jab and the flu vaccine are the No. 1 and No. 2 most dangerous injections respectively, based on adverse event reports and payouts from the U.S. Vaccine Injury Compensation Program. Both are also capable of shedding, and both can make you more prone to infection as their protection wears off
COVID-19 has been going on for nearly three years, and with a whole new set of untested COVID boosters being rolled out, some scientists are taking a step back, cautioning that there still are unanswered questions about how the shots work.
They say more research needs to be done on what is known as “original antigenic sin,” aka “immune imprinting,” which refers to how your immune system responds to repeated introductions of the COVID variants.
Understanding Original Antigenic Sin
The following description of original antigenic sin was published in a January 2019 Journal of Immunology paper titled “Original Antigenic Sin: How First Exposure Shapes Lifelong Anti–Influenza Virus Immune Responses”:1
“The term ‘original antigenic sin’ (OAS) was first used in the 1960s to describe how one’s first exposure to influenza virus shapes the outcome of subsequent exposures to antigenically related strains. In the decades that have passed, OAS-like responses have been shown to play an integral role in both protection from and susceptibility to infections.
OAS may also have an important deterministic role in the differential efficacy of influenza vaccine responses observed for various age cohorts across seasons …
OAS describes the phenomenon whereby the development of immunity against pathogens/Ags is shaped by the first exposure to a related pathogen/Ag … subsequent infections with similar influenza virus strains preferentially boost the Ab response against the original strain …
The critical role of primary exposure in shaping the composition of the Ab repertoire was not only observed in humans after influenza virus infections; this phenomenon was also observed in animal models and in the context of other infectious agents.
For example, additional serum absorption experiments in ferrets infected in succession with three different influenza virus strains demonstrated that nearly all of the host Abs after the infection series were reactive against the first strain, only a fraction of serum Abs could be absorbed by the secondary virus, and fewer yet by the tertiary virus.”
Simplified Example
Here’s a layman’s summary to illustrate this phenomenon as simply as possible, within the context of COVID:
- Exposed to the original Wuhan SARS-CoV-2 strain, your humoral immune system is programmed to produce antibodies against that specific virus. Similarly, if you got the jab, your body will produce antibodies against the viral spike protein formulated into that shot.
- Exposed to the Delta strain, your immune system responds first by boosting production of the original antibodies, while antibodies specific against Delta are produced in a far lower amount as it takes time for your body to respond to the new strain.
- Exposed to an Omicron variant, your immune system again responds by boosting the original antibodies, while antibodies against Omicron are produced in even lower amounts than those against Delta.
As a result of this process, with each exposure to a new variant, the original antibodies get “back-boosted.” So, over time, those antibodies come to predominate.
The process is (at least theoretically) the same for all vaccinations. Each booster dose back-boosts or strengthens the original antibodies, making them more and more predominant. The problem is that they may not be effective at neutralizing newer strains (depending on the amount of mutation), thus rendering you more and more prone to symptomatic infection.
Frequent Boosting May Backfire
As reported by ABC News:2
“Some experts say they are concerned that frequent boosting with the original version of the vaccine may have inadvertently exacerbated immune imprinting. At this point in the pandemic, some adults have received four or more doses of the same vaccine …
[Some] scientists worry about a potential backfire, with frequent boosting handcuffing the body’s natural immune system and leaving it exposed to radically different variants that might emerge in the future.
‘Where this matters is if you keep giving booster doses with [original] strain, and continue to lock people into that original response. It makes it harder for them to respond then to essentially a completely different virus,’ says Dr. Paul Offit, professor of pediatrics at Children’s Hospital Philadelphia …
The timing of vaccines may also need to be taken into account, as the nation moves from original doses to updated boosters.
‘It is true that the best boosts typically are the ones that are given infrequently, that immunologically, if you boost too much and too frequently, then you often have a lower immune response at the end,’ said [director of the center for virology and vaccine research at Beth Israel Deaconess Medical Center, Dr. Dan] Barouch.”
Data Confirm Negative Efficacy After Second Dose
In the video above, Dr. Meryl Nass reviews official data from the U.S. Centers for Disease Control and Prevention, which confirm that people who got two or three COVID jabs are MORE likely to get ill with COVID six to eight months after the last dose than had they gotten none.
Should You Double Up on COVID Booster and Flu Shot?
Our reckless health authorities are potentially worsening matters further by pushing people to simultaneously get the updated bivalent COVID booster and a seasonal flu vaccine this fall.

Early in September 2022, White House medical adviser Dr. Anthony Fauci urged Americans to “Get your updated COVID-19 shot as soon as you are eligible,” and White House COVID coordinator Ashish Jha, September 6, stated, “I really believe this is why God gave us two arms, one for the flu shot and the other one for the COVID shot” — a statement that will live on in infamy as one of the most ridiculous comments from a public health official ever uttered.3
One problem, although hardly the most important one, is that it’s still far too early for a flu shot. As noted by STAT News:4
“The protection generated by influenza vaccines erodes pretty quickly over the course of a flu season. A vaccine dose given in early September may offer limited protection if the flu season doesn’t peak until February or even March, as it did during the unusually late 2021-2022 season.
‘If you start now, I am not a big fan of it,’ Florian Krammer, an influenza expert at Mount Sinai School of Medicine in New York, told STAT. ‘I understand why this is promoted, but from an immunological point of view it doesn’t make much sense.’”
STAT cites research showing the effectiveness of the flu shot wanes by about 18% for every 28 days’ post-vaccination. What it doesn’t mention is the fact that the flu shot historically has had an effectiveness well below 50% to start with. The 2018/2019 flu vaccines, for example, which outperformed the 2017/2018 vaccines, had an adjusted effectiveness rating of:5
- 29% for all ages
- 49% for children aged 6 months through 8 years
- 6% for children ages 9 through 17
- 25% for adults between the ages of 18 and 49
- 12% for those over 50
This May Become the ‘Dark Winter’ Biden Warned About
Ever since the rollout of the COVID shots, there have been suspicions that some kind of shedding is happening between the jabbed and the unjabbed.6 With mass flu vaccination, the possibility of transmission is further exacerbated, and there’s no telling what kind of viral mutations the combination of a bivalent COVID jab and a quadrivalent flu shot might produce.
A study7 published January 18, 2018, in the journal PNAS showed that people who receive the seasonal flu shot and then contract influenza excrete infectious influenza viruses through their breath.
What’s more, those vaccinated two seasons in a row had a greater viral load of shedding influenza A viruses. According to the authors, “We observed 6.3 times more aerosol shedding among cases with vaccination in the current and previous season compared with having no vaccination in those two seasons.”
This study also highlighted the possibility that annual flu vaccination might lead to reduced protection against influenza over time, and that each vaccination can make you progressively more prone to getting sick. That, again, is the original antigenic sin phenomenon discussed above.
Now, combine the possibility of antigenic sin for COVID with the antigenic sin for influenza, and what might we end up with? Who knows? Research8 has also shown that priming your immune system with influenza vaccine can make you more susceptible to bacterial infections as well, and what are face masks loaded with? Bacteria.
Taken together, we could well be facing the “dark winter” president Biden warned would befall the unvaccinated last year. But it’ll be those with COVID booster and quadrivalent flu shots who will suffer the most. The rest of us will hopefully avoid problems provided we keep our immune systems strong.
Both Shots Are Associated With Serious Side Effects
On top of the antigenic sin possibility for both the COVID jab and the flu vaccine, there’s the possibility of suffering serious side effects from either or both of these shots. Before the advent of the COVID jab, injury following influenza vaccination was the most compensated claim in the federal Vaccine Injury Compensation Program (VICP).
Between January 1, 2006, and December 31, 2019, a total of 5,407 injury claims for flu vaccine were filed, 4,614 of which were compensated.9 Based on VICP injury filings and awards, the flu vaccine was the riskiest vaccine out there. The COVID jab, however, blew the flu shot out of the water within the first few weeks of use.
“This fall, they’re telling people to line up for the two riskiest and deadliest injections out there. Media are stating that getting the flu shot and the COVID jab at the same time is ‘safe.’ Yet there are absolutely NO data to support such a claim.”
As of September 2, 2022, just 21 months into the COVID jabs existence, 1,400,350 post-jab injuries have been reported to the Vaccine Adverse Event Reporting System (VAERS).10 That’s more than half of all VAERS reports collected for all vaccines since its inception 32 years ago.
So, this fall, they’re telling people to line up for the two riskiest and deadliest injections out there. In my view, this is reckless beyond belief, and I would caution against this strategy. Disturbingly, media are stating that getting the flu shot and the COVID jab at the same time is “safe.”11 Yet there are absolutely NO data to support such a claim. It’s pure assumption.
Vaccine Journal Warns of Serious Side Effects
The fact that the COVID jabs can cause serious side effects is evident by VAERS data alone, but studies reanalyzing original trial data submitted to the U.S. Food and Drug Administration are also starting to emerge that confirm the riskiness of these shots.
Most recently, a study12 13 in the journal Vaccine concluded the Pfizer and Moderna COVID jabs are associated with a 16% “excess risk of serious adverse events of special interest” over placebo baseline, on average. As detailed in that paper:14
“In 2020, prior to COVID-19 vaccine rollout, the Brighton Collaboration created a priority list, endorsed by the World Health Organization, of potential adverse events relevant to COVID-19 vaccines. We adapted the Brighton Collaboration list to evaluate serious adverse events of special interest observed in mRNA COVID-19 vaccine trials.
Methods: Secondary analysis of serious adverse events reported in the placebo-controlled, phase III randomized clinical trials of Pfizer and Moderna mRNA COVID-19 vaccines in adults … focusing analysis on Brighton Collaboration adverse events of special interest.
Results: Pfizer and Moderna mRNA COVID-19 vaccines were associated with an excess risk of serious adverse events of special interest of 10.1 and 15.1 per 10,000 vaccinated … respectively. Combined, the mRNA vaccines were associated with an excess risk of serious adverse events of special interest of 12.5 per 10,000 vaccinated …
The Pfizer trial exhibited a 36 % higher risk of serious adverse events in the vaccine group; risk difference 18.0 per 10,000 vaccinated … The Moderna trial exhibited a 6 % higher risk of serious adverse events in the vaccine group: risk difference 7.1 per 10,000 …
The excess risk of serious adverse events found in our study points to the need for formal harm-benefit analyses, particularly those that are stratified according to risk of serious COVID-19 outcomes. These analyses will require public release of participant level datasets.”
Researchers Call for Release of Patient Data
In an open letter addressed to the CEOs of Pfizer and Moderna published in The BMJ,15 the authors of this Vaccine paper call for the release of all clinical data, including individual participant data, so that a more thorough reanalysis can be made:
“The effort to prepare these datasets is minimal, and no potentially identifying data is needed … Today (Aug 31), our study of serious adverse events in the Pfizer and Moderna phase 3 COVID-19 vaccine trials was published in the peer-reviewed journal Vaccine.
The results showed the Pfizer and Moderna both exhibited an absolute risk increase of serious adverse events of special interest (combined, 1 per 800 vaccinated), raising concerns that mRNA vaccines are associated with more harm than initially estimated at the time of emergency authorization.
We acknowledge that our estimates are only approximations because the original data remain sequestered. For example, we could not stratify by age, which would help clarify the populations in which benefits outweigh harms.
A more definitive determination of the actual harms and benefits requires individual participant data (IPD) that remain unavailable to research investigators … COVID-19 vaccines are now among the most widely disseminated medicines in the history of the world.
Yet, results from the pivotal clinical trials cannot be verified by independent analysts. The public has a legitimate right to an impartial analysis of these data …
Transparency, reproducibility, and replication are cornerstones of high-quality science. The time is overdue for Pfizer and Moderna to allow independent scientists and physicians to see the original data and to replicate the analyses.”
COVID Jabs Linked to Excess Deaths
The COVID shots also appear to be responsible for the rapid increase in excess deaths around the world. As reported September 8, 2022, by The Defender,16 the COVID jabs are causing injuries on a scale we’ve never seen before in medical history.
Yet governments around the world are turning a blind eye. Most medical researchers also avoid these data like the plague, for fear of getting defunded. Two university professors in Germany, however, have bucked that trend.
Psychologist Christof Kuhbandner and Matthias Reitzner, a statistician, analyzed excess mortality data from the German Federal Statistical Office (Bundesamt für Statistik) for 2020 through August 2022.17 18
By applying actuarial analysis to the all-cause mortality data — i.e., by estimating the number of all-cause deaths during these years had there been no pandemic, and then comparing that to the observed all-cause deaths — they found the death toll in 2020, at the height of the pandemic, was actually close to the expected number.
In 2021, however, the observed number of deaths were “two empirical standard deviations above the expected number.” What’s more, the increase in mortality only started to accumulate after April that year. A similar pattern was also observed for stillbirths, which rose by 11% in the second quarter of 2021.
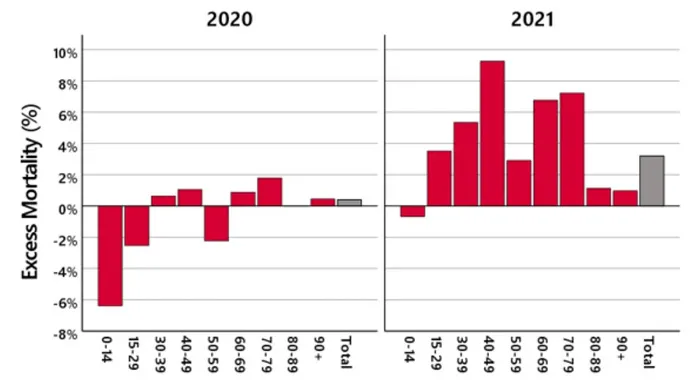
The figure below illustrates the differences in excess mortality between 2020, the year of the virus, and 2021, the year of the COVID jabs.19 20 Looking at the age groups, we see something very odd. In 2021, excess mortality was highest among 15- to 79-year-olds, yet COVID infection primarily killed the elderly, 70 to 79 years of age, in 2020.
Mortality in age groups 15 to 29, and 50 to 59, during the pandemic, pre-jab, was actually below average, and excess mortality among children was well below average. Yet in 2021, excess mortality went up for all age groups, not just the elderly. This strongly suggests the COVID virus was not a primary contributor, but rather the experimental injections.
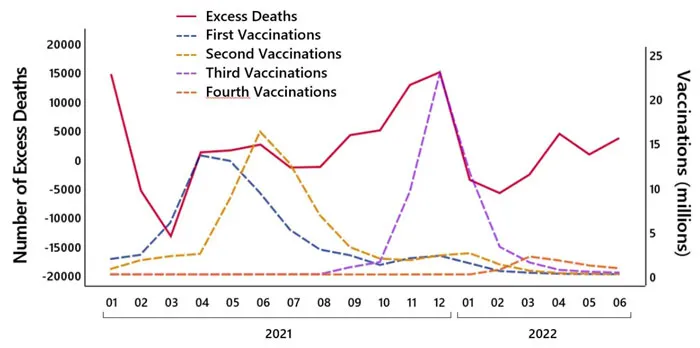
Kuhbandner and Reitzner further notes there were spikes in excess mortality in April and May and again in September, November and December 2021. The April/May spike coincides with the COVID shot rollout in Germany, and the increases in the fall correlate with booster campaigns.
Don’t just survive — THRIVE! Prepper All-Naturals has freeze-dried steaks for long-term storage. Don’t wait for food shortages to get worse. Stock up today. Use promo code “jdr” at checkout for 25% off!
The following graph21 22 illustrates how tightly connected the excess mortality numbers are with the rise and fall in COVID shots administered.
In my view, there’s simply no doubt the COVID jabs are causing more harm than good, and combining a reformulated and never tested bivalent COVID booster with a quadrivalent flu shot could potentially be disastrous.
It’s becoming increasingly clear that fiat currencies across the globe, including the U.S. Dollar, are under attack. Paper money is losing its value, translating into insane inflation and less value in our life’s savings.
Genesis Gold Group believes physical precious metals are an amazing option for those seeking to move their wealth or retirement to higher ground. Whether Central Bank Digital Currencies replace current fiat currencies or not, precious metals are poised to retain or even increase in value. This is why central banks and mega-asset managers like BlackRock are moving much of their holdings to precious metals.
As a Christian company, Genesis Gold Group has maintained a perfect 5 out of 5 rating with the Better Business Bureau. Their faith-driven values allow them to help Americans protect their life’s savings without the gimmicks used by most precious metals companies. Reach out to them today to see how they can streamline the rollover or transfer of your current and previous retirement accounts.


The government, the CDC, NIH have totally bastardized the medical industry! With all the horror the covid vaccines have created, how can anyone have any faith or trust in doctors and the medical community about anything!
Occam’s Razor: The solurion with the minimum number of assumption is the more likely solution.
The explanation as proposed in the above explanation…OR…your immune system is so occupied dealing with a foreign protein the jab has programmed YOUR OWN CELLS TO MANUFACTURE, that it can no longer deal with viruses that once was v routinely suppressed. Your body only has a limited number of ways to deal with a virus. It finds a virus….it responds. The mRNA jab programs cells to produce the spike protein….instead of the proteins it needs to repair/maintain itself….eventually it dies….new jab, new cells programmed. Regardless of what the tests claim, subsequent “covid” infections are really other viruses instead. You don’t really catch a cold. Cold viruses are routinely suppressed by gamma-globulins that are temperature sensitive. Mammals constant body temperatures maintain the gamma-globulin effectiveness. But get a chill, and the viruses are released. Run a fever and gamm-globulin effectiveness is increased and the viruses are put bat in the box. The mRNA jab makes your immune system ineffective in a similar, yet parallel, way.
Which explanation includes the most facts and the fewest assumptions? You decide.
We’re too late. The double jab + booster jab was enough for a majority that took it. Some may need a second booster jab to complete the process. Destroy natural immunity and depopulation will commence.
All part of the plan, along with AIDS.
No mask, no jabs, no problem.
Never follow the delusional anywhere.